Bodi Empowerment
5 Common Misdiagnoses of TMJ Pain: And Why Getting It Right Matters

Please follow and like us:
TMJ pain is frequently mistaken for headaches, ear infections, nerve disorders, or sinus problems. Here’s how to tell the difference and what a proper diagnosis actually involves.
If you’ve been living with unexplained jaw pain, facial pressure, ear fullness, or chronic headaches, you may have already seen multiple providers without clear answers. You’re not alone. Temporomandibular joint (TMJ) disorders are among the most commonly misdiagnosed conditions in musculoskeletal medicine and the reasons why have everything to do with how pain travels through the head and neck.
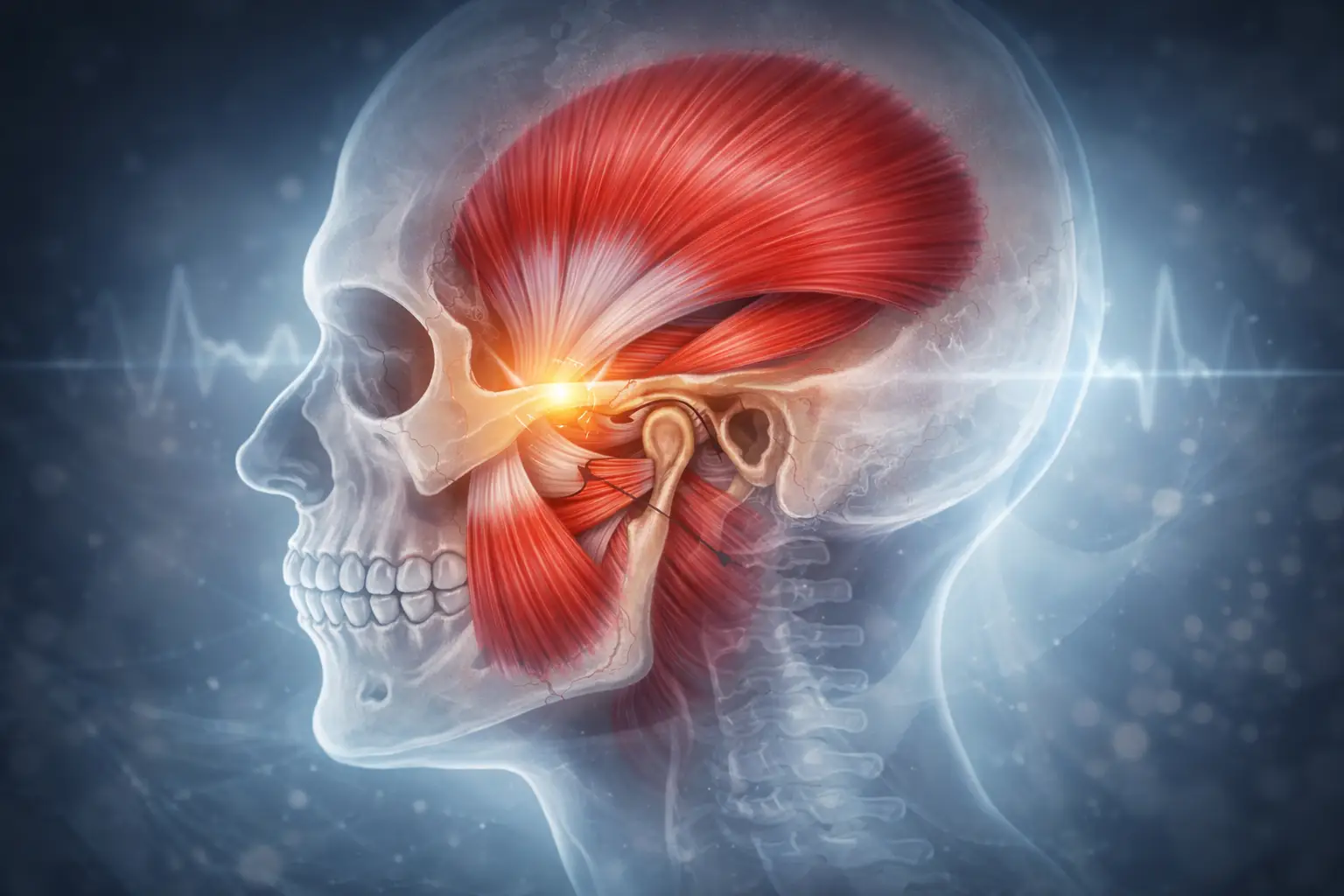
The TMJ sits at the crossroads of the jaw, ear, cervical spine, and trigeminal nerve system. When something goes wrong in this region, symptoms can appear almost anywhere in the face, skull, or throat. That’s why TMJ disorder is often confused with everything from migraines to sinus infections to ear disease.
Understanding these overlapping conditions and what sets them apart is essential for anyone seeking lasting relief from jaw or facial pain.
1. Cervicogenic Headaches: When Neck Dysfunction Looks Like TMJ Pain
One of the most frequently missed diagnoses in patients presenting with jaw and facial pain is cervicogenic headache a condition where dysfunction in the upper cervical spine generates referred pain into the temples, jaw, and face.
The upper three cervical segments (C0–C3) share neurological pathways with the trigeminal nerve, which is responsible for sensation in the face and jaw. This anatomical overlap means that joint restriction, muscle tightness, or nerve irritation in the neck can produce symptoms that feel identical to a TMJ problem.
Symptoms that suggest cervicogenic involvement:
- Jaw tightness or aching that worsens with prolonged sitting or screen use
- Temple headaches or pressure behind the eyes
- Pain or discomfort when chewing that fluctuates with neck position
- Morning jaw stiffness accompanied by neck stiffness
- Postural headaches that begin at the base of the skull and radiate forward
Many patients with this pattern see significant improvement when the cervical spine is treated directly even without any specific jaw intervention. A thorough evaluation that includes the neck is essential before assuming the problem is purely mechanical jaw dysfunction.
2. Trigeminal Neuralgia: Nerve Pain That Mimics Dental and Jaw Disorders
Trigeminal neuralgia is a neurological condition involving the trigeminal nerve the same nerve that supplies sensation to the face, jaw, and teeth. Because of this anatomical overlap, patients with trigeminal neuralgia are sometimes told they have a dental problem or a TMJ disorder before the correct diagnosis is made.
The key differentiator is the nature of the pain itself. Trigeminal neuralgia typically presents as:
- Sudden, electric, or stabbing pain often described as shock-like
- Episodes triggered by light touch: brushing teeth, chewing, speaking, or a light breeze on the face
- Very short-lived bursts seconds to a minute but extremely severe
- Pain localized along the cheek, jaw, teeth, gums, or lips
Unlike most TMJ disorders, trigeminal neuralgia is primarily a neurological condition often related to vascular compression of the nerve root and requires medical investigation, including imaging. While chiropractors who specialize in head and neck conditions can contribute to the broader assessment, neurological management is central to this diagnosis.
3. Myofascial Pain Syndrome: When the Muscles, Not the Joint, Are the Source
Not all jaw pain comes from the temporomandibular joint itself. In many cases, the actual source is myofascial — meaning that tight, overloaded muscles surrounding the jaw are generating referred pain into the teeth, temples, ears, and even down into the neck.
The primary chewing muscles the masseter, temporalis, and medial and lateral pterygoids can develop trigger points: hyperirritable nodules within the muscle tissue that refer pain in predictable patterns far from the tender spot itself.
Myofascial jaw pain often presents as:
- A dull, persistent ache in the jaw or cheeks
- Headaches concentrated at the temples
- Fatigue when eating hard or chewy foods
- Tenderness to palpation of the facial muscles
- Symptoms that worsen with stress, teeth clenching, or bruxism
This condition is particularly common in people who clench during sleep, those with high stress loads, and individuals with forward head posture. Because myofascial pain is muscle-driven rather than joint-driven, it often responds well to manual therapy, dry needling, and postural correction not splints or joint-focused interventions.
4. Ear Disorders: Why TMJ and Ear Symptoms Are So Easily Confused
The temporomandibular joint sits directly in front of the ear canal, separated from it by only a thin bony wall. This proximity means that TMJ dysfunction frequently produces ear symptoms and equally, that ear pathology can mimic jaw problems.
Patients with undiagnosed TMJ disorders often cycle through audiology and ENT referrals before the jaw is identified as the source. Conversely, true ear pathology can produce facial and jaw symptoms that prompt an unnecessary TMJ workup.
Ear-region symptoms commonly linked to TMJ dysfunction:
- Ear pain without infection or structural finding on examination
- A persistent feeling of fullness or pressure in the ear
- Tinnitus — ringing, buzzing, or hissing in the ear
- Mild vertigo or imbalance, particularly with jaw movement
A useful diagnostic clue: if an ENT examination is entirely normal but ear symptoms persist, the jaw and surrounding musculature deserve careful evaluation. The tensor tympani and tensor veli palatini muscles both involved in Eustachian tube regulation share nerves with the muscles of chewing, which may explain the ear-jaw symptom connection.
5. Sinus Problems: Facial Pressure That Isn’t Always Sinusitis
Maxillary sinus inflammation is a well-known cause of facial pain, cheek pressure, and upper tooth sensitivity. But the reverse is also true: jaw dysfunction and myofascial tension in the facial muscles can generate symptoms that closely resemble sinusitis even when the sinuses themselves are entirely clear.
This creates a diagnostic trap. Patients presenting with cheek pressure, facial heaviness, and upper jaw aching may be treated with repeated antibiotics or nasal corticosteroids, only to see limited improvement. When imaging fails to show sinus pathology, the musculoskeletal system deserves a closer look.
Sinus-like symptoms that may have a musculoskeletal origin:
- Diffuse facial pressure or heaviness that worsens through the day
- Upper tooth sensitivity with no clear dental cause
- Pain in the cheeks and temples that worsens with jaw use
- Headaches that increase when bending forward — but don’t respond to decongestants
The pterygoid muscles, which run through the infratemporal fossa adjacent to the maxillary sinus, are a common source of referred facial pressure. Trigger points in these muscles can produce symptom patterns that are virtually indistinguishable from sinusitis on history alone.
Why Accurate TMJ Diagnosis Requires a Whole-System Approach
TMJ disorders rarely present as isolated mechanical problems. In clinical practice, most complex or chronic jaw pain cases involve some combination of:
- Joint dysfunction or disc displacement
- Cervical spine restriction, particularly at C1–C3
- Myofascial trigger points in the jaw, neck, and shoulder girdle
- Central sensitization an amplified nervous system response to ongoing pain
- Parafunctional habits such as clenching, bruxism, or postural loading
This is why a thorough assessment must go beyond the jaw joint itself. Evaluating cervical range of motion, palpating the musculature of the face and neck, assessing bite mechanics, and understanding a patient’s postural habits all contribute to identifying the true drivers of the problem.
Clinicians trained in both spinal and craniomandibular evaluation are well-positioned to identify these overlapping contributors and to coordinate care with dentists, neurologists, and ENTs when warranted.
When Should You Seek a Professional Evaluation for Jaw Pain?
Many people delay seeking care for TMJ symptoms because the pain comes and goes, or because they’ve been told nothing is structurally wrong. Early assessment matters — not because all jaw pain becomes chronic, but because long-standing TMJ dysfunction is more likely to generate secondary problems including cervicogenic headache and widespread facial pain.
Consider a musculoskeletal evaluation if you experience any of the following:
- Jaw pain or facial aching that persists beyond two weeks
- Clicking, popping, or catching sensations in the jaw with movement
- Headaches that appear to originate from the jaw or temples
- Ear symptoms pain, fullness, or ringing without infection
- Difficulty opening the mouth fully, or jaw deviation on opening
- Upper tooth sensitivity with no clear dental explanation
- Facial pressure that does not respond to standard sinus treatment
The Bottom Line on TMJ Misdiagnosis
TMJ pain is a diagnosis that demands context. The jaw does not function in isolation it is biomechanically, neurologically, and anatomically connected to the cervical spine, the ear, the sinuses, and the entire craniofacial musculature. When clinicians treat the jaw in isolation, they risk missing the conditions that are actually driving the symptoms.
A comprehensive evaluation one that assesses movement patterns, cervical function, muscle tenderness, and symptom triggers together gives patients the best chance of an accurate diagnosis and a treatment plan that produces lasting results.
If you have been living with jaw pain, headaches, or unexplained facial symptoms and have not yet had a musculoskeletal assessment, it may be the missing piece in your care.
Dr. Ken Nakamura is a Certified Chiropractic Sports Practitioner (CCSP) with specialized training in TMJ disorders, cervicogenic headache, and concussion. For more information, visit bodiempowerment.com.
Please follow and like us:


Dr. Ken, has been recognized as the Best Toronto Chiropractor in 2024, 2023, and 2018, here in downtown Toronto. As a sports chiropractor, he excels in treating a wide range of conditions including concussions, temporomandibular joint disorders (TMJ), sports-related injuries, and spinal issues. Beyond his clinical skills, Dr. Ken is an accomplished athlete, having represented Ontario in the Canadian Judo Championships and completed the Toronto Marathon on two occasions. He employs the innovative C3 Program to provide targeted and effective care to his patients, ensuring a holistic approach to their well-being and athletic performance.