Bodi Empowerment
Hip //
Overcome Hip Impingement Syndrome: What You Need to Know

Do you have a groin or hip pain while tying your shoes, or going up the stairs?
Does sitting for long periods make your pain worse?
Does your pain sometimes become sharp or “catch” with activity?
If you answered yes to these questions you might have hip impingement syndrome. The technical name for this condition is femoral acetabular impingement syndrome.
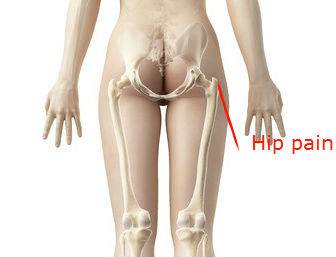
You also might be walking with a swing of your torso over the bad side, and feeling pain right over your hip. Keep in mind most people will feel the pain as in the diagram above not near the belt-line.
Symptoms of Hip Impingement / Femoral Acetabular Impingement Syndrome.
Best Exercises For Your Supraspinatus
- Pain in the groin area sometimes radiates to the thigh or knee.
- Hip pain like in the picture above aggravated by activity
- Buttock pain
- Clicking of the hip
- You are a teenager to forty years of age
Most of you would have had physiotherapy or chiropractic without any positive results. X-ray reports came back negative for the hip, and groin ultrasounds didn’t show anything wrong. (Just because pain is located near the groin doesn’t necessarily imply that it’s a groin pull.
Your doctor, your physiotherapist, and, most importantly, you are frustrated that you can’t engage in much activity before starting to experience hip pain.
Hip impingement syndrome is related to abnormalities of the hip or using the hip in extreme ranges of motion.
Abnormalities Of The Hip
Abnormalities of the hip joint can occur in one of two places. Your hip joint is a ball and socket joint. The abnormal shape can be at the ball part of the joint or the socket end.
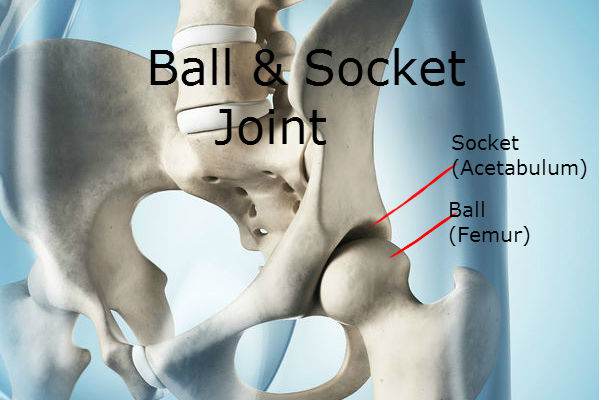
The socket is known as the acetabulum, and the ball is referred to as the femur head.[7-9]
Here I go over some of the abnormalities not visible on the X-ray followed by those abnormalities visible on the X-ray.
Piriformis Syndrome: The Best 6 Exercises To Help Your Hip & Butt Pain
Causes Hip Impingement or Femoral Acetabular Impingement Syndrome Not Visible On X-rays
- Acetabular (acetabulum) retroversion is a condition where the socket portion of the hip joint is angled more backward than is typical. Generally, most individuals have their sockets slightly facing forward. However, if the socket points more backwards, then acetabular retroversion is present. Intriguingly, this is a congenital condition. Often, individuals with this anomaly may have one foot pointing outward, or in cases where both sides are affected, both feet may point outward[10].
- Acetabular Retroversion can be detected on X-rays; however, it is frequently overlooked, leading me to categorize acetabular retroversion as often “non-visible” on X-ray. The oversight occurs because many radiologists may not be familiar with hip impingement indicators or may not actively search for them. When identified, a distinctive “cross-over sign” is visible, although interpreting this sign accurately requires specific training.
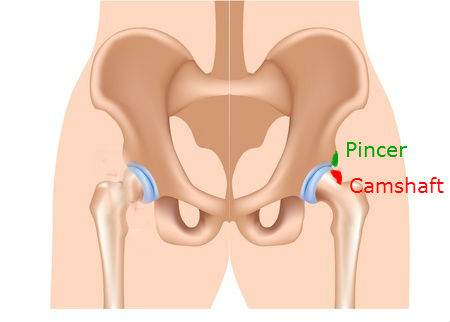
- Moving on, the Camshaft (Cam) Deformity involves excess bone growth on the femur’s upper surface[11]. Individuals with a Cam deformity typically experience pain during hip flexion, especially when the hip rotates inward.
- Similarly, the Pincer Deformity is characterized by excess bone growth on the acetabulum’s upper lip, leading to significantly restricted hip flexion and inward rotation.
- Frequently, individuals exhibit a combination of both camshaft and pincer deformities, with the camshaft deformity highlighted in red and the pincer deformity in green in the accompanying diagram.
- Additionally, a previous fracture to the femur (thigh bone) can alter the ball-and-socket joint’s alignment, impacting the hip’s function.
Causes Of Hip Impingement Visible On X-ray
One cause is Slipped Femoral Epiphysis, a condition where the femur’s ball end slips backwards due to a weakness in the growth plate, often resulting in pain during adolescence.
Another cause is Legg-Calvé-Perthes disease, which occurs when the femur’s ball loses blood supply, leading to bone death. This condition primarily affects children.
A common misconception is that X-rays, which may appear normal or show minor issues like a small spur on the acetabular rim, downplay the seriousness of the condition.
However, the real issue arises during hip movement, where the pincer deformity can jab into the joint, resembling a fork puncturing the cartilage. This repeated action can cause cartilage damage and tears on the femur’s ball surface.
Such tears lead to abnormal hip movements and, over time, contribute to the wear and tear of the hip joint, culminating in premature osteoarthritis, often before it typically occurs in one’s peer group.
Impingement Test

http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2293316/
One test will be positive for 90% of you who have this condition. It’s called the impingement test. Make sure your healthcare practitioner does this test.
Your healthcare provider will have you lying down on your back.
- Flex your hip to 90 degrees.
- The knee is then adducted (pushed past the midline), while internally rotating the hip
When the test is positive you will know as you will feel a pain that is sharp in the area of your hip or recreates the pain they usually have.
Feel free to share your questions, thoughts and experiences in the comments below, and don’t forget to connect with us on Facebook for more updates and tips on improving your health. We’d love to hear your opinions on who you consider the best Toronto chiropractor.
Research
1 . Ganz R , Parvizi J , Beck M , Leunig M , Notzli H , Siebenrock KH . Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Rel Res . 2003; 417: 112 – 20. [PubMed]
2 . Kassarjian A, Yoon LS, Belzile E, Connolly SA, Millis MB, Palmer WE. Triad of MR arthrographic findings in patients with cam-type femoroacetabular impingement. Radiology. 2005; 236: 588 – 92.[PubMed]
3 . Ito K, Minka MA, Leunig M, Werlen S, Ganz R . Femoroacetabular impingement and the cam effect: an MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br . 2001;83: 171 – 6. [PubMed]
4 . Ito K, Leunig M, Ganz R . Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Rel Res . 2004; 429: 262 – 71. [PubMed]
5 . Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R . Anterior femoroacetabular impingement: part 2. Midterm results of surgical treatment. Clin Orthop. 2004; 418: 67 – 73. [PubMed]
6 . Goodman DA, Feighan JE, Smith AD, Latimer B, Buly RL, Cooperman DR . Subclinical slipped capital femoral epiphysis. J Bone Joint Surg. 1997; 79: 1489 – 97. [PubMed]
7 . Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M . Anterior femoroacetabular impingement: part 1. Techniques of joint preserving surgery. Clin Orthop Rel Res . 2004; 418: 61 – 6.[PubMed]
8 . Tanzer M, Noiseux N . Osseous abnormalities and early osteoarthritis: the role of hip impingement.Clin Orthop Rel Res . 2004; 429: 170 – 7. [PubMed]
9 . Wagner S , Hofstetter W , Chiquet M , Mainil-Varlet P , Stauffer E , Ganz R , et al. Early osteoarthritic changes of human femoral head cartilage after femoroacetabular impingement. Osteoarthritis Cartilage. 2003 ; 11 ( 7 ): 508 – 18 . [PubMed]
10. D. Reynolds, J. Lucas, K. Klaue. Retroversion of the acetabulum: A CAUSE OF HIP PAIN. J Bone Joint Surg. 1999
11 . Peters CL, Erickson JA. Treatment of femoral-acetabular impingement with surgical dislocation and debridement in young adults. J Bone Joint Surg. 2006; 88A: 1735 – 41. [PubMed]
Related Categories: Hip, Low Back Pain, Surgery

Dr. Ken, has been recognized as the Best Toronto Chiropractor in 2024, 2023, and 2018, here in downtown Toronto. As a sports chiropractor, he excels in treating a wide range of conditions including concussions, temporomandibular joint disorders (TMJ), sports-related injuries, and spinal issues. Beyond his clinical skills, Dr. Ken is an accomplished athlete, having represented Ontario in the Canadian Judo Championships and completed the Toronto Marathon on two occasions. He employs the innovative C3 Program to provide targeted and effective care to his patients, ensuring a holistic approach to their well-being and athletic performance.