Bodi Empowerment
Acupuncture //
Managing Disc Bulge: Effective Strategies for Pain Relief

Do you have a disc bulge that is causing you incredible pain in your lower back?
Does your disc bulge give you sciatica or pain down your leg?
Have you wondered what’s going on in your lower back to cause all this pain?
In this issue of Bodi Empowerment, I go over what’s going on with your disc bulge, the cause of your pain and what kind of treatments are best for you. In other words, I act as a guide to help you decide what to do.
Disc herniations, or disc bulges occur when the disc that is found between vertebrae in the spine is damaged. Most of the time the damage occurs in stages.
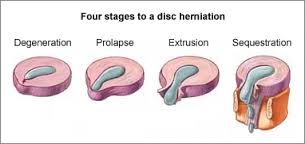
Here are the four stages of a disc herniation or disc bulge:
- Disc Bulge
- Disc Prolapse
- Disc Extrusion
- Disc Sequestration
Think of the disc as a flat hard onion with strawberry jelly inside. The jelly is the nucleus while the onion layers form circular layers of hard cartilage called the annulus.
Disc Bulge
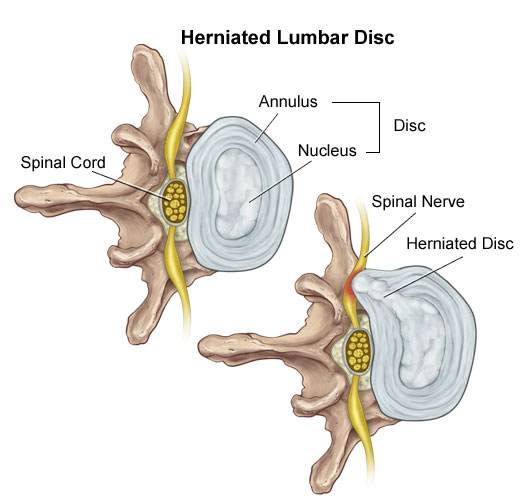
If you were to damage the annulus (onion) enough the disc gets to a point that when you bend forward, you pinch the front of the onion so it starts to bulge the onion at the back by pushing the nucleus (jelly) backwards.
This is called a disc bulge. For most of you, there is no pain but for some of you, there can be considerable lower back pain and even sciatica from this small disc bulge.
Disc Protrusion
A disc protrusion is like a disc bulge that comes out even more in one focused spot. The disc pushes out as if you had your finger inside a balloon and pushed out.
Most of the layers of the onion (annulus) have been damaged but the jelly (nucleus) is under considerable pressure. The jelly (nucleus) squeezes through the layers of the annulus (onion) with the few intact layers of the onion (annulus) and the PLL (posterior longitudinal ligament) holding the jelly from spilling out. The disc is still contained by the annulus and PLL ligament. ie the balloon hasn’t popped.
Disc Protrusions usually cause quite a bit of lower back pain and often times sciatica. Many of you, with disc protrusions, on the other hand, have absolutely no pain. There is no clear reason. A study found that 40% of people with no pain whatsoever had disc protrusion confirmed by MRI (Magnetic Resonance Imaging Machine) [1]
The trick is not to let your doctor diagnose you based on just an MRI. An MRI that shows a disc protrusion by itself is not a diagnosis. It’s what a normal person with no pain can have. Make sure there is other evidence!
Disc Extrusion
Disc Extrusion is a disc bulge so large that it breaks through the last layers of the onion (annulus) and the PLL ligament pushing into the area of the spinal cord. ie. The balloon has popped. If you have an extrusion you likely have a tremendous amount of pain leg pain and usually some lower back pain.
Surprisingly when a group of normal people with no pain were scanned with an MRI 18% were found to have disc extrusions (severe disc herniations). [1]
When you have a disc extrusion chances are the extrusion is likely causing your pain as it’s so large.
Disc Sequestration
Disc sequestration occurs when a piece of your jelly (nucleus) that breaks through the onion (annulus) and the PLL ligament has now broken off and moved away further into the spinal cord area. When you have a disc sequestration you have a tremendous amount of leg pain and some lower back pain.
Smaller Is Better: Disc Bulge
Disc Herniations or slipped discs are better if they are smaller, right? You will have less pain right? Yes except when they give you pain. Remember all those normal people with no pain with all kinds of slipped discs? They had disc bulges, disc protrusions, and disc extrusions and even disc sequestrations with no pain.
On the other hand, even with a small disc bulge, you can get a lot of pain and even sciatica with no pressure on the nerve. So smaller isn’t always better.
Bigger Is Better: Disc Bulge
Sometimes bigger is better. Most people like you with disc extrusion and sequestration have lots of pain. The fact is these painful extrusions while more painful usually shrink with time. It takes about a year but with the shrinking of the herniations, the pain does decrease.[2-5]
Disc Herniation: Disc Bulge Treatment
#1 Stop Aggravating Yourself
Half the problem why people don’t get better is that they continually aggravate their lower back and their slipped discs. Learning to lift properly, sit properly and even stand over the sink while brushing your teeth properly can help you avoid the pain.
Even Yoga exercises such as the downward dog can aggravate the lower back, Pilates and even your basic abdominal crunch have been shown by Dr Stuart McGill to increase the pressure in the disc beyond its safe limit.
If you want to find out how to stop aggravating your lower back, click the link below.
See Also: Slipped Discs: Best Self-Treatments To Help Your Lumbar Disc Herniation
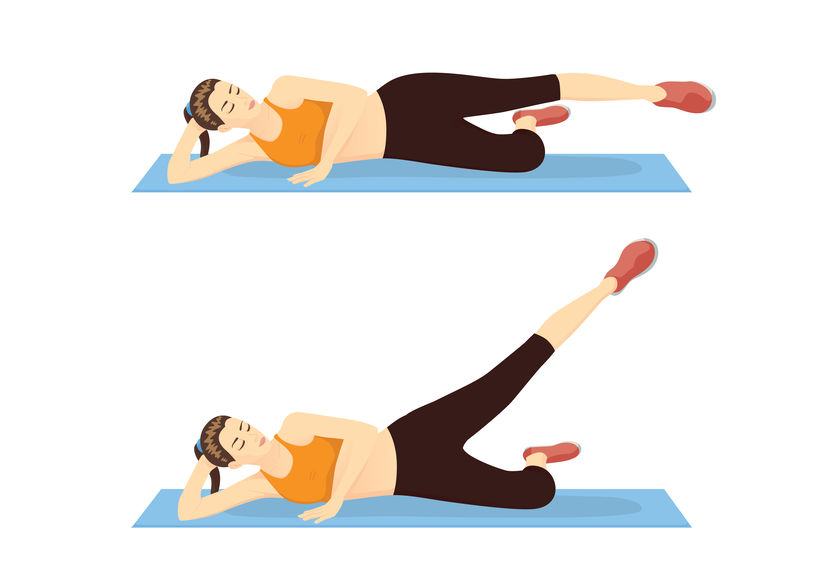
#2 Exercise For Disc Herniations / Slipped Discs
For complete instructions on exercises for slipped discs click the link. Best Exercises For Your Slipped Disc
#3 Chiropractic Adjustments For Disc Bulge
A major research paper showed that people who have had lumbar disc herniations who have failed at least 3 months of medical management, including treatment with analgesics, lifestyle modification, physiotherapy, massage therapy, and/or acupuncture, should consider chiropractic spinal manipulative treatment, followed by surgery if unsuccessful. [6]
I would also add that I would try 3 different chiropractors as the competency level varies from person to person. Like any profession including medical doctors and physiotherapists, there are the good ones and bad ones.
See also: 6 Things You Should Look For In A Chiropractic Clinic
#4 Acupuncture For Disc Bulge
Acupuncture is helpful for Slipped Discs in the neck and the lower back.[7-8]
#5 Injections
In a study of two different groups getting treatment for lumbar disc herniations, the group getting chiropractic manipulation had 76.5% of the people improve while the group getting the nerve root injections improved by 62.7%.
After a month, the chiropractic spinal manipulation group had a 60% reduction in pain compared to the nerve root injection group, which had a 53% decrease in pain. Keep in mind the nerve root injection group seemed to be worse to start with compared to the spinal manipulation group.
See Also: Chiropractic Spinal Manipulation Vs. Nerve Root Injections for Lumbar Disc Herniations
Epidural injections are also helpful for lower back pain and the radiating pain down your leg.[8]
#6 Surgery
#1 Discectomy
There are two types of surgery available for slipped discs. Discectomy and spinal fusion. This surgery involves cutting out the piece of the disc that is protruding out and pushing on the spinal cord or nerve.
Discectomy is relatively simple compared to spinal fusion. You have a much better chance of success with discectomy if your MRI shows that your disc herniation is greater than 7 mm thick and correlates well with your neurological exam and nerve conduction studies.[9] If your lower back pain is greater than your leg pain discectomy will not likely work very well for you.[10]
#2 Spinal Fusion
Spinal Fusion removes the disc herniation, jelly (nucleus), and most of the annulus (onion). Bone from the pelvis is then transplanted where your disc was so that the two vertebrae become one.
What Treatment Should You Do?
You should do at least 3 months of therapy when you have a slipped disc before even considering surgery or injections. Start by not aggravating your lumbar disc. You need to modify how you bend forward, lift and even pick up your socks.
See Also: Disc Herniation: Best Self-Treatments To Help Your Lumbar Disc Herniation
If you have trouble sleeping at night you can take painkillers to help you get a better sleep. Don’t stay in bed though. When you have excruciating pain you should only have bed rest for a maximum of two days total.
Next, try chiropractic or physiotherapy with someone who also does acupuncture. Make sure it’s not with somebody who knows how to do 20 acupuncture points. Be patient with them as disc herniations can be difficult to deal with.
Attend regularly 3 times a week for at least a month. Make sure they change the treatments to find what works best for you. If they keep doing the same thing each visit but you are improving that is fine, but if you aren’t improving then it’s time to find a new chiropractor.
If you don’t get any better after a month change to a different chiropractor. I recommend trying 3 different chiropractors as different chiropractors have different training.
If you plateaued or haven’t improved at all then it’s time to get a nerve root injection or an epidural injection. Make sure it’s with a person that does this every day. An emergency room doctor or family physician only does this procedure once in a while. It’s better to get someone more experienced.
When conservative care has been completely exhausted then it’s time to consider surgery. Discectomy is more conservative than spinal fusion and recovery is much quicker. You should consider discectomy surgery if you have :
- Foot drop that is getting worse.
- Any other neurological symptoms that is getting worse like your reflexes, sensitivity
- Bowel or Bladder Symptoms (loss of your poo and pee function). : This is an emergency you should go to the hospital right away.
- If you have a disc protrusion or that is 8 mm or larger that correlates well with a neurological exam, and Nerve conduction tests.
- Leg pain is worse than your lower back pain.
Beware of the surgeon who wants to operate on a small disc bulge. There are too many unnecessary surgeries in the USA especially spinal fusion.
Spinal fusion is considered when your lower back pain is worse than your leg pain
Tell us what you think in the comments below and like us on Facebook. This Toronto Downtown Chiropractor will answer all questions in the comments section.
Research
1. Weishaupt D et al. “MRI of the lumbar spine: Prevalence of intervertebral disc extrusion and sequestration, nerve root compression and plate abnormalities, and osteoarthritis of the fact joints in Asymptomatic Volunteers.” Radiology – 1998; 209:661-666
2. Maigne JY, Rime B, Delignet B. Computed tomographic follow-up of 48 cases of nonoperatively treated lumbar intervertebral disc herniation. Spine 1992; 17:1071-1074.
3. Ikeda T, et al. Pathomechanism of spontaneous regression of the herniated lumbar disc: histologic and immunohistochemical study. J Spinal Disord 1996;9:136-140.
4. Ahn SH, Ahn MW, Byun WM. Effect of transligamentous extension of lumbar disc herniations and their regression in the clinical outcome of sciatica. Spine 2000; 25:475-480.
5. Komori H, Shinomiya K, Nakai O, et al. The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996; 21:225-229.
Research
6. McMorland G et al.Manipulation or microdiskectomy for sciatica? A prospective randomized clinical study. Journal of Manipulative & Physiological Therapeutics 2010; 33: 576-584.
7. Wu, Yao-chi, Jun-feng Zhang, Yi-jun Sun, Cheng-fei Huang, Ping Shao, and Gui-zhen Liu. “Clinical study on electroacupuncture for cervical intervertebral disc herniation.” Journal of Acupuncture and Tuina Science 11, no. 6 (2013): 371-374. – See more at: http://www.healthcmi.com/Acupuncture-Continuing-Education-News/1249-acupuncture-found-superior-to-drug-for-neck-disc-pain#sthash.vD0pNepM.dpuf
8. Wang HeshanNon-Surgical Therapy For Prolapse of Lumbar Intervertebral Disc. The Journal of Traditional Chinese Medicine
9. Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in managing chronic low back pain and lower extremity pain: a systematic review. Pain Physician 2009;12:163-188.
Research
10. Carragee EJ, et al “Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment types and annular competence” J Bone Joint Surg Am – 2003; 85(1):102-108
11. McMorland G et al.Manipulation or microdiskectomy for sciatica? A prospective randomized clinical study. Journal of Manipulative & Physiological Therapeutics 2010; 33: 576-584.


Dr. Ken, has been recognized as the Best Toronto Chiropractor in 2024, 2023, and 2018, here in downtown Toronto. As a sports chiropractor, he excels in treating a wide range of conditions including concussions, temporomandibular joint disorders (TMJ), sports-related injuries, and spinal issues. Beyond his clinical skills, Dr. Ken is an accomplished athlete, having represented Ontario in the Canadian Judo Championships and completed the Toronto Marathon on two occasions. He employs the innovative C3 Program to provide targeted and effective care to his patients, ensuring a holistic approach to their well-being and athletic performance.




Hi Doc Ken I’m Ferdinand age 23yrs and I must say you are doing a great job helping people to recover from back pain and slip disc.
Doc three months back I had miserable back pain and due to travel I neglected it. Gradually it started hurting my buttocks and tingling feeling behind my calf.
3months past and I just got tested recently.The doc told me to perform some movements to test and said its minor slip disc. He then suggested me to go for an MRI.
MRI report:
L4 is partially dessicated and normal in height. A broad based posterior central disc protsuion with annular fissure is seen at l4-5 which indents the anterior aspect of the thecal sac and the l5 traversing nerve roots in the epidural space as they exit the sac.
Please help am really worried.
1)Is it a serious case??
2)Am a football player .. Will I be able to play again??
3)How much time approx will it take to cure??
Author
Thanks for your question Ferdinand. First keep in mind that what your MRI says and the cause of your back are often different. As an example 30% of 30 year olds have disc herniation but they don’t have any symptoms when checked by MRI. Hopefully your medical doctor or whoever examined you are not diagnosing by MRI and that they actually did a great examination and careful history of your problem.
1. If the cause of your pain is your disc then it’s not serious but something to be concerned about.
2. If you are talking about soccer then you can play earlier than if you are playing American or Canadian type of football.
3. You can see that the time to be “cured” depends on the diagnosis. If you pain is due to a disc it may take a few weeks to a few months but a lot of it depends on how much you aggravate the problem and how diligent you are about doing your exercises. Also if you have any other conditions or diseases and if you are sitting in your job or if you are student and sitting a lot. Thus the very wide time frames. I have some people that come to me and they’ve had pain for 6 months, or even a year. It depends on a lot of factors.
You can also do these exercises. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
Like all exercises you can make your lower back worse. If the pain, numbness or tingling goes further down the leg then you are getting worse. That means you need to stop the exercises. The exercises should be supervised by a health professional at least at the beginning.
Hope that helps your disc herniation.
Hello doctor.
i am Turjo, now 21 years old.
17 months ago, i tried to lift some heavy things, and suddenly i felt pain in my lower back.
i can’t sit on chair for long. and, my RIGHT foot having some problem also. foot pain is much less than lower back pain.
Doctor recommended an MRI saying:
1. Posterior disc protrusion seen at central-paracentral L4-5 level causing anterior thecal sac indentation.
2. Disc desiccation seen at L4-5 level with reduction of height at L4-5 level
3.Screening of cervical and dorsal spine appear unremarkable.
and, i was given prgabalin, omeprazole, indometacin, nortriptyline for a long time, which i don’t thing works anything.
i am a student of computer science, and sitting and programming is a must for me, which i do having a belt recommended by doctor. what will u suggest for me for cure.
i want to be a normal person with no pain on sitting and on foot.
Author
Thanks for your question Turjo. That’s quite a cocktail of drugs you’ve got there. First for the vast majority of people shouldn’t wear a belt. The belt will eventually weaken your core making you dependent on it to keep you out of pain. The better way is to make your own back by strengthen your own muscles surrounding your lower back, abdomen and buttock muscles. This will help your present pain and help prevent problems.
You should try these exercises. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
Like any exercises they can make you worse. If the pain, numbness or tingling goes further down the leg then you are getting worse and need to stop. You should have these exercises supervised by a chiropractor or other professional.
Hope that helps your disc herniation.
Author
This is the same answer I gave you in another article in which you commented on.
Thanks for your question Turjo. That’s quite a cocktail of drugs you’ve got there. First for the vast majority of people shouldn’t wear a belt. The belt will eventually weaken your core making you dependent on it to keep you out of pain. The better way is to make your own back by strengthen your own muscles surrounding your lower back, abdomen and buttock muscles. This will help your present pain and help prevent problems.
You should try these exercises. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
Like any exercises they can make you worse. If the pain, numbness or tingling goes further down the leg then you are getting worse and need to stop. You should have these exercises supervised by a chiropractor or other professional.
Hope that helps your disc herniation.
Helo sir I have a problem with l4-5 diffuse posterior disc bulge with thecal sac identition .and l5-s1 disc extrusion disc bulge please provide me a link of exercise. And consult me .thankyou
Author
Thanks for your question Gaurav. I can’t give you exercises as you haven’t told me anything regarding your pain. 30% of 30 years olds have disc herniation but no back pain.
Hope you understand.
Dear Sir,
i’m from India and need adcice for my mother who is 60 yrs old. She is facing acute pain in both her legs which starts from her toes and reaches her hips. She also feels numbness in her legs when she stands for about 20 minutes at a stretch.
she was prescribed LUMIA K,CHOLECALCIFEROL (VITAMIN D) ONCE IN A WEEK and
her mri scan rebealed the following report which i share with you for proper advice and treatment. Waiting for your reply..
mri scan report –
1) a transitional vertebra at the lumbosacral junction,which has been labelled as L5.it appears sacrilozed.L5-S1 disc is rudimentary.
2) diffuse bulge,with right foraminal protrusion of L4-5 disc.
3) mild diffuse bulge of L3-L4 disc.
4) ligamentum flavum thickeneing and facetal arthropathy at L4-L5 level.
please advice accordingly.
thank you
Rajesh babu
Author
Thanks for your question Rajesh. She may benefit from these exercises but she was born with a rudimentary disc. https://www.bodiempowerment.com/spinal-stenosis-comprehensive-guide-5-exercises-spinal-stenosis-lateral-stenosis/
Like any exercise they can make you worse. They should only be done with supervision of a health care provider.l
Hope that helps your mother;s leg pains
Hi Doctor Ken,
For the past 15 years I have severe pain in my lower back specially when I walk 1-2 kilometres or stand for 40 – 60 minutes or bend down to pick something and also when i wake up in the morning. Pain has significantly increased in the last 2 years. The neurologist has advised me for leminectomy surgery as the only solution.
Here is my MRI report (done on 1.5 Telsta machine):
L5-s1 disc reveal diffuse posterior bulge with medium sized posterocentral protrusion compressing thecal sac and indenting budding nerve root along with ligamentum falvum thickening causes moderate canal stenosis.
I am scared of the surgery as at times its fails. Please advise….
Regards,
Safdar Ali,
Bahrain.
Author
Thanks for your question Safdar. Your problem is complicated enough that you need professional help. You should see your local chiropractor or physiotherapist in your area. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
These exercises may help but they might make you worse. Remember the exercises should be supervised by a health professional. You will know if you are getting worse if the pain increases or the numbness, tingling or pain goes further down the leg. If this happens you should stop the exercises.
Hope that helps your disc herniation.
Dear Dr.Ken , In process of searching proper advise I luckily find your Web site ,I read your Articles and believe me Sir….I felt that You had written lot of helpful things for all like us (who are experiencing lack of knowledge,and suffering great pain ) Sir ,I am Bindu san , woman ,Age 40,Indian, working professional experiencing lower back pain from last 5 years and during this period I consulted more than 4 orthopedic surgeons to get rid of my lower back pain but the result is not very fine.Although the medicines, nerobion injections,vitamin suppliments and physiotherapic exercises reduced my pain for some time but not completely removed so I am in search of proper advise for my pain treatment.I will be higly oblidged if you can suggest me something for this..please..
Recently I did my MRI (SCAN OF LUMBER SPINE)the rediologists report is as follows :-
MRI SCAN OF lumber spine was performed using T1/T2W Sequences in multiple planes .in additional sagittal T2W Screening of whole spine has been obtained.
Partial Sacralisation of L5 Vertebra is noted (counting has been from scanogram) minimal scoliosis of the lumber spine is seen towards left side.mild exaggerated lumbar lordosis is noted.mild degenarative lumber spondylotic chages are seen in the form of marginal osteophytes.disc dessication is seen at L3-L4 and L4-L5 levels. Minimal posterior disc bulge is seen at L2-L3 Level. diffuse posterior annular disc bulge is seen at L3-L4 Level, prtially affecting anterior subarachnoid space without significant nerve root compression. moderate diffuse posterior disc herniation is seen at L4-L5 Level, effacting anterior subarachnoid space,eccroaching upon neural foramina,significantly compressing thecal sac-intrathecal nerve roots both transerving L5 Roots (R>L) and indenting existing L4 nerve roots. mild degenarative facetal arthropathy and ligamentam flavum thickning is noted at this level-further contributing to lumber spinal canal narrowing.bilateral mild neural foramnam narrowing -bilateral moderate lateral recess narrowing (R>L) and moderate Spinal canal stenosis (8.5 to 9.0 mm) is noted at L4-L5 level crowding of intrathecal nerve root at L4-L5 level. degenarative facetal arthropathy and ligamantum flavum thickning is seen at L3-L4 and L4-L5 levels (more marked t L4-L5 Level) MR Myelography reveals mild extradural indentation at L3-L4,L4-L5 levels. sacral spinal canal cyst is noted at s1/s2 level mesuring 3.9×4.0x1.5 cm(CC x RL)
Distal cord and conus appear normal.both hip and SI joints are normal. no pre/paravertebral,epidural soft tissue or haematoma is seen. bilateral psoas and posterior paraspinaous muscles are normal. visualized pelvic bones appear normal. THE WHOLE SPINE SCREENING :-no significant abnormality is seen in the dorsal spine screening. Mild straightening of cervical spine curvature is noted.minimal posterior disc bulge is seen at C3-C4 level. mild posterior annular disc bulge is seen from C4-C5 to C6-C7 levels. spinal cord appears normal. no abnormal cord signal or cord compression is seen . atanto -axial joint appears normal.
Sir . the MRI Report is as above . I am working professional which required 6-7 hours seating work . I hardly find any other time for exercises. but regularly do physiotherapists suggested exercises and find that the exercises help me to lessen some pain but it is not complately gone away. I want to leave good life. I want to become pain free so please advise me what should i do ? the back pain rediates from my lower back to right leg (knee to heel ) some time i felt like cramps in my leg and I can hardly walk more than 15 minutes there after the pain rediates more and more. so please suggest me what should i do ? is my MRI Says I AM A CASE OF SURGERY ? is there not any option other than spine surgery ? can it be treat by lessor therapy ? or my problem can be solved by any other therapy / treatment ? some people says that the INJECTIONS IN SPINE can relieve my pain….what would you suggest…? please advise. I will be highly oblidged if you can guide me for further treatment. i am eagerly awaiting your kind reply…please advise….
Author
Thanks for your question Bindu San. You can try these https://www.bodiempowerment.com/posture-correct-your-exaggerated-low-back-arch/
Like any exercises they can make you worse so should be supervised by a health professional.
Also try some massage on the leg.
Hope that helps your disc herniation.
Hey doc… Its a real pleasure that you are helping patients like this.
I, too, is a victim of disc bulging & suffering from severe pain that just keeps getting better with rest & worse with daily activities. I first noticed this pain almost 3 months back with just mild bending during daily activities. It was a point near my L5 at left side. Then within a week it just got so worse that it was hard for me to even walk or move. The pain started to travel down my left leg too. I got myself an MRI and it showed:
Left foraminal disc protrusion at LV4-5 level causing indentation of thecal sac only with narrowing of left lateral recess and compression of ipsilateral nerve root.
My neurosurgeon kept me on muscle relaxants analgesics and all other medications possible in this case but now after 2 months these don’t seem to effect me. I am on the physiotherapy too but I don’t think its helping me much. They use TENS machine on me now. After it sometimes it doesn’t pain and when it pains its way too bad. Excruciating pain starts every time I do any sort of walking or anything & now even when I sit the pressure on the buttocks aches me. This wasn’t the thing before and now my leg pain is worse than my back pain.
I’ll be highly obliged if you help me with my problem.
I HAD AN MRI RECENTLY AND THE RESULT WAS AT L5 S1 THERE IS A MILD DEGENERATIVE LOSS OF DISC HEIGHT WITH LOSS OF DISC SIGNAL. AT L5 S1 THERE IS A SMALL BROAD BASED RIGHT PARACENTRAL DISC PROTRUSION WHICH IS IN CLOSE PROXIMITY WITH THE ORIGIN OF THE RIGHT S1 NERVE ROOT i WILL REALLY APPRECIATE IF YOU CAN ANSWER MY QUESTION .
CAN I STILL DO MY JOB. I WORK AS A HEALTH CARE AIDE IN A NURSING HOME AND THERE IS SOME LIFTING INVOLVED AS I OPERATE THE LIFTS AND STAND AIDE.. THANKS DOCTOR
Author
Thanks for your question Jessica. You should really read this article to stop aggravating your disc herniation. https://www.bodiempowerment.com/disc-herniation-part-1/
If you stop aggravating your disc you will be more likely able do your job. Ask your health practitioner that examined as I haven’t examined you or taken a history.
Hope that helps your disc.
Dear Dr Ken,
I am Satish from India. Few Days before I felt some pain in my leg and it started increasing day by day. When I Got my M.R.I. then I came to know that there is problem with L3-L4, L4-L5 and L5-S1. Below are some points which are mentioned on M.R.I. Report:
1. Lumbar Spondylosis
2. Diffuse posterior annular bulge with right para central protrusion of L4-L5 disc material causing central canal stenosis with right lateral reccess stenosis and compression of right L5 traversing nerve root.
3. Diffuse posterior annular bulge at L3-L4 and L5-S1 levels along with ligamentum flavum hypertrophy causing central canal stenosis with partial effacement lateral reccesses.
Kindly suggest me what should I do. I am diabetic patient and from last few months my Blood pressure in also on the higher side ranging from 150 to 190.
Kindly help.
Author
Thanks for your question Satish. You can try these exercises. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
However like any exercise they can make you worse. That is why the exercises need to be supervised by a chiropractor or other health practitioner. You know you are getting worse if the pain increases or the pain or any other symptom like numnbess, tingling or pain starts going further down the leg.
Hopetat helps your lumbar spondylosis.
Dear Dr. Nakamara,
I’ve been experiencing low back pain and numbness in the front of my right thigh for about 2 weeks now, after having been thrown from a treadmill in April and recently spending hours on long car rides. I’m also a runner and an accordionist.
My MRI yesterday reveals the following results:
L1-L2: Small broad based right foraminal disc protrusion. Mild narrowing of the right neural foramen. Central canal and left neural foramen are patent.
L2-L3: Small superiorly extruded right forminal disc herniation with herniated disc material measuring up to 8 mm in diameter which impinges on the exiting right L2 nerve root. Central canal and left neural foramen are patent. Right neural foramen is moderately narrowed.
L3-L4: Minimal diffuse disc bulge. Central canal is patent. Mild bilateral neural foraminal narrowing.
L4-L5: No disc bulge or herniation. Mild facet joint hypertrophy Central canal is patent. Mild bilateral neural foraminal narrowing.
L5-S1: Tiny central disc protrusion. Mild facet joint hypertrophy. Central canal is patent. Mild bilateral neural foraminal narrowing
Conus: Normal size and signal. Terminates at approximately L1
Impression: Mild lumbar spondylosis with small disc herniations at L1/2, L2/3, and L5/S1 Disc herniation is largest at L2/3 and is located at the right neural foramen with impingement on the exiting right L2 nerve root.
I am able to walk without pain. There is no problem with bowel or bladder control, but the nerve pain in my groin and leg is keeping me up at night. Neurontin doesn’t touch the pain. I’ve developed positional vertigo from sleeping on my left side….the only side I can rest “comfortably” on. I’ve stopped all running, of course. Walking helps. I’ve started PT and have not been in it long enough to assess whether or not it’s going to work. My PCP suggests an Ortho consult. I’m afraid I may need surgery. Your comments?
Thank you in advance for any advice you can give me. Your website is very informative!
Sincerely,
Marilyn
Author
Thanks for your question Marilyn. You have quite a large disc herniation at L2-L3. The good news about disc extrusions is that they often get reabsorbed by the body but the process can take 6 months to a year.
You have groin area pain due to the pinched nerve that leads to the groin area. The only problem is the exercises I can give you will likely aggravate you.
https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
I wouldn’t do the cobra but you might try the sphinx. If the pain gets worse or if the symptoms go further down the leg with feelings pain, numbness or tingling than you are getting worse. You have to have the exercises supervised by a health professional.
Hope that helps your disc herniation.
Thank you for your prompt response! The pain is excruciating at night, beginning at about 5:30 and I can’t imagine dealing with it for 6 months! I’ve had to talk myself out of going to the ER. I plan to consult a neurosurgeon at Yale to see whether surgical intervention is an option for me. I need this to stop.
Author
Thanks for your comment Marilyn. I would try a good chiropractor or physiotherapist. The good news is that for disectomies a type of disc surgery your disc which is sticking out 8mm is more likely to be successful. Any less than 8mm and it is usually less successful according to the research. If surgery is recommended I would get a second opinion especially if they suggest fusion surgery. The complications are worse, takes more time to recover and it’s done too often according to the Washington Post citing the goverment’s own records.
It’s always better to do conservative therapy first before surgery.
Hope that helps your disc herniation.
Hello Sir,
Below is my MRI details:
L3 – L4 disc shows diffuse annular bulge wit small posterior protrusion causing moderate to severe narrowing of neural foramina and mild indentation of left exiting, bilateral traversing nerve roots.
L4 – L5 shows broad based posterior protrusion causing indentation of thecal sac, filar roots, severe narrowing of neural foramina and mild compression of exiting, traversing nevre roots (L > R)
L5 – S1 disc shows diffuse annular bulge causing mild narrowing of neural foramina and mild compression of exiting nerve roots.
Moderate narrowing of spinal canal opposite L4, L5
Well circumscribed lesion (1.9 X 1.3 cms) hypointense on T1, heterogeneously isointense on T2 and hyperintense on STIR
Please let me know is MRI shows any serious issues. What should be my next steps to follow.
Thanks,
Naresh
Author
Thanks for your question Naresh. I can’t answer your question without you telling me what your pain is like. You see MRI and pain don’t correlate often. A thorough history and exam is needed more often then an MRI.
Hope you let me know what your symptoms are for your lower back.
Sir,
I do have pain at lower right back since 2 months. Sometimes its severe when I work or lie down on bed for a long period and sometimes its very mild.
Majorly, may be due to pain or any other reason my upper body has been tilted towards left a bit.
Thanks,
Naresh
Author
Thanks for your question Naresh. Your L4-L5 disc is the likely culprit. I haven’t diagnosed you as I haven’t examined and I am only going by the information on hand.
You can do these exercises for your problem. https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
Any exercise can hurt you. These exercises should be supervised by a health practitioner accordingly. If the pain gets worse or you get symptoms going down into the buttock like numbness, tingling or pain than you are getting worse and so should stop the exercises.
Hello doctor sen,
for the past few months i was suffering from pain in my lower back in my buttocks and thighs. after i went to doctor he suggested for mri. in MRI scan the impressions are as follows
L5-S1:
Diffuse disc bulge with prosterior disc protrusion causing narrowing of central canal and bilateral neural foraminawith compression over bilateral traversing and exiting nerve roots.
L4-L5:
Diffuse disc bulge causing of bilateral neural foramina and compression over bilateral traversing and exiting nerve roots.
I want to ask you dear sir that is it a serious problem? sir please tell me with complete information of every single word, at which position my disc is bulged out.
Another thing i want to tell you that i have pain at my upper back also when i sit to study and sometimes in my neck and in shoulder. Is this means that do i have thoracic disc bulge also. if not than what might be the cause of this problem. please answer sir..please
Author
Thanks for your question Yash. There are a couple of assumptions here. The cause of the lower back pain is on the MRI. When MRIs are done on normal people with no back pain 30% of 30 years are found to have disc herniations.
Assuming that your doctor did a thorough exam and history and made a diagnosis before the MRI and didn’t do the typical diagnosis by MRI, then you have a quite a problem but usually one that can be helped by exercises.https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
The exercises should be done under supervision of a health care provider as any exercise can make you worse.
Hope that helps your possible disc herniation.
Hi Doctor Ken, I am a 56 year old and have many surgeries for different things not related to disc problems.
For the last 3 years I have had a numbness in my lower legs and feet, and pain down to arms. I have a disc bulge on the C5,6,7 and a disc bulge with headaches and pain in face, and also I have a a disc bulge with material extruding onto the spinal cord in the L5. I have had spasms down the body since Sept last year. i have been referred to a Neuro Surgeon. Over the last couple of years I have had physio, chiro, acupunture and bowen therapy. I have also had two falls in the last six months one 6 weeks ago. Last night i had a severe pain in my lower back, with pain down to the legs and arms. What can I do?, Thank you
Author
Thanks for your question Lee. You have a complicated problems which can only be addressed with a proper history and exam done in person. There are too many factors to take into account and too many assumptions that would be made without face to face contact.
Hope your disc bulges get better.
Thanks for the immediate response Dr. Ken. I am from India and yes I did pay a pretty sum for my scan and to consult the doctor. The MRI scan lasted about 30 minutes and my doctor did an examination and advise for say 15 min. Is there any complications involved in my situation doctor? Please advise.
Hi Dr. Ken,
First of all I would like to appreciate your patience in answering to all of us coming to you with our problems. I am 24 years old and I am diagnosed with slip disc since last week. My MRI reports have the following impression :
1) Disc dessication with bulge and posterior central protrusion at L5 S1 level causing mild impingement on the ventral thecal sac and the bilatetal traversing nerve roots.
2) Disc bulge at L4-5 level with the disc margin just touching the exciting nerve roots outside the foramen.
I am married and work for a software company and I am very much concerned about what happened to me. Please suggest me on what are the possible effects to my life style and what are the possible remedies. Is there a permanent cure for this apart from surgery? Would I be able to ride my bike and get back so normal so I was before? Please advise.
Author
Thanks for your question Thilak. You should try these exercises provided that the disc is the cause of the problem.https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
If the problem is related to your disc than you will likely get rid of your pain and it will likely come back. Why sitting too much and you likely aggravate your own problem. Read about how not to aggravate your own disc herniation. https://www.bodiempowerment.com/disc-herniation-part-1/
I have questions for you:
1. Did your doctor do a thorough history and exam? >10-15 minutes
2. Did you pay for the MRI and the visit to the doctor?
3. Which country are you from?
Hope that helps your possible disc herniation.
Thank you Doctor Nakamura,
#1 I ment “Lift your heels off the floor while keeping your toes on the floor and your knees straight. ” Is it OK for her condition? Thank you!
Author
Thanks for your question Irina. Likely this will be difficult for her but if not she should have the back of the chair to hold onto so she doesn’t lose her balance.
Hope that helps her slipped disc, osteoporosis etc…
Dear Doctor Nakamura,
Thank you so much for doing this great job to help those who suffer pain. Hopefully you will kindly give me advice too. My mother is 90 years old. Although she has osteoporosis for a while, she is pretty active, attends a swimming pool, walking.
• The acute pain suddenly appeared on the left of her low back, especially when she stood up.
• She felt pain going down to her leg immediately after low back pain so that she even was unable to put weigh on her left foot for some times.
• Besides, when she straightens her left leg, she felt some discomfort and tension in it. When she went to bed, it was easier to lie on the left side for some reason..
• She did not feel any pain while walking although the pain got aggravated at her body turns.
• Under any other circumstances, pain did not bothered her and almost gone in 2 weeks except some episodes when she turned in the bed.
Family doctor prescribed her ibuprofen and Lidocaine patches 5%
MRI findings:
Examination of lumbar spine shows mild straightening of normal lumbar lordosis. There is Chronic-appearing compression deformity involving T12, L2&L5 vertebral bodies with 10-15% loss of vertebral body height. No marrow edema is seen to suggest acute to subacute compression fracture. Degenerative endplate changes and desiccation are noted through lumbar spine. There is no spondylosis. Conus medullar is is at its normal location of L1 level. No abnormal signal is seen within the conus.
L2-L3: Right–sided disc-bulge and bilateral facet arthrosis with right-sided neural foramina narrowing and mild central canal stenosis. No gross nerve root compression.
L3-L4: There is broad-base disc bulge and bilateral facet arthrosis is causing mild to moderate central canal stenosis and bilateral neural foramina narrowing. Bulging disc is seen contacting left exiting L3 nerve root at this level
L4-L5: There is diffuse disc bulge and bilateral facet arthrosis causing moderate central canal stenosis and left for standby bilateral neural foramina narrowing. No definite nerve root compression is seen
There is no gross Para spinous soft tissue abnormality
MRI Report
L5-S1: The is central disc bulge and bilateral facet arthrosis causing moderate central canal stenosis and bilateral neural foramina narrowing
MRI impression
1. Degenerative disc bulge and bilateral facet arthrosis causing mild to moderate central canal stenosis and bilateral neural foramina narrowing
2. Chronic appearing compression deformity involving T12, L2, and L5 vertebral bodies. No acute compression fracture or spondylosis’s
***
Considering her age, we would be interested in:
1. Which exercises would you kindly recommend for her in terms of the further treatment and prevention?
2. How not to aggravate her condition in order to avoid potential pain attacks?
Any advises would greatly appreciate!
Irina
Author
Thanks for your question Irina. While MRI are getting better they cannot see everything. For example only 12% of disc herniations can you see the actual tear of the outer part of the disc called the annulus, but for more serious disc herniations is assumed to be that there is a annular tear.
So while there is no “recent” compression fracture it is a likely possibility based on symptoms. The other is a disc herniation although less likely due to the short lived nature of the problem.
Although there are a lot of disc bulges, central stenosis and pinching of the nerves in various places most of them are not likely causing her the pain.
She can do these exercises but she cannot do them without professional supervision. If you try to save money and not have someone supervise her you will likely cause her further injury due to her age and her fragility. All exercises can do her harm especially in this case.
https://www.bodiempowerment.com/part-2-degenerative-disc-disease-exercises-help-lower-back-pain-spondylosis/
All the exercises are too hard for her and would need to be modified for her.
Hope that helps her low back pain.
Dear Doctor Nakamura,
My mother and I really appreciate your response. She did not even believe that somebody would concern about such an elderly patient.
It sounds, that there is a plenty of risk even with the physical therapist supervision as it is definitely about qualifications…..Anyway I will do my best trying to find the right one. Thank you so much!
At the moment please allow me to ask couple of more questions:
1. My mother attends adult care facility where they do some general exercises. It sounds like they stand on toys up-down. Is it OK for her or she should avoid this kind of exercises?
2. When in adult care, she attends a swimming pool twice a week. Is it OK for her (she is not a swimmer actually). What kind of activity would be beneficial to do while in a swimming pool? Real swimming or just moving or anything else?
3. How to stand up in order not to cause more pain going forward?
4.Is it a lot to walk for 30 minutes w/o break? What is an optimal pattern?
Thank you very much in advance. Any advice is very desirable and appreciated!
Irina
Author
Thanks for your questions Irina.
1. ? “stand on toys up-down
2. She should walk and float and easy strokes if she can do it easily.
3. Try to keep the curve in your lower back when you stand.
4. Walk what you can. If she is up to 30 minutes without a break that is great. As long as she has her balance. There is no optimal.
Hope that helps her low back pain.
Dear Doctor Nakamura,
Thank you for all your generous help and consideration! I hate to bother you again, but I would like to make sure that I have a clear understanding of my elderly mother’ problem. So far my understanding is:
1. This is not a big probability that my mother’s pain was caused by disk herniation, disk bulge or even central stenosis.
2. Due to her symptoms and MRI restrictions there is a probability that there might a recent fracture due her osteoporosis .
I know that it is not for sure and that it is really simplified, but do I at least have a feeling in a right direction? Thank you so much in advance!
Irina
Author
Thanks for your questions Irina. Yes that is what I am thinking but remember that I haven’t examined your mother and I don’t have a full history. That’s my opinion based on the information I have so far. I wouldn’t call it a dignosis though just an opinion.
Hope that helps your mother’s back problem.
Sir, in Jan 2015 during playing football I hv injured myself, came to know only after 48 hr, a severe pain in my lower back. my MRI findings are A POSTERIOR DISC BUGLE WITH A LEFT SIDED PROPENSITY AT L4-L5
LEVEL CAUSING MARKED NARROWING OF BILATERAL LATERAL RECESSES
(LEFT>RIGHT) WITH COMPRESSION OF THE BILATERAL TRAVERSING
NERVE ROOTS AND MILD EFFACEMENT OF THE THECAL SAC .
• A SMALL POSTERIOR DISC BULGE AT L5-S1 LEVEL CAUSING MILD
EFFACEMENT OF THE THECAL SAC.
Please correlate
Author
Thanks for your question Sushant. If your doctor would do a thorough exam and history you can get the right treatment. People with no pain have disc herniations ie 60% of 60 years old have disc herniations. You can try these exercises assuming that the problem is a disc herniation but it is no guarantee.
https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
You can do the exercises above but as I said your diagnosis is up in the air. You should have the exercises supervised by a health professional like a chiropractor. If the exercises cause increased pain or causes pain to go down into the leg or further down or give you symptoms like numbness, tingling or pain than you should stop the exercises.
Hope that helps your possible disc herniation.
Hello Doctor,
I’m Jaya from India. I had disk bulge l5-s1 about 1 and half years ago. It took 5 months to recover and the pain went away by exercise and ice. After 1 year, today I got the disk bulge pain back. What should I do doctor? I feel devastated to go through the pain again !! Please help!!
Author
Thanks for your question Jaya. Unfortunately you have found out that back pain for most people comes back from time to time. You must be vigilant to prevent the problem form recurring.
This article is all about prevention and how to stop aggravating your lower back problem from the most common type of disc herniation.
Hope that helps your disc bulge.
Dear Dr.Ken.
I have been suffering from low back pain since many years. I am an active person and go for jogging, walking, and also do other exercises. I am 54 yrs. Normally the pain comes and goes off after I continue to do all the stretching exercises as recommended by you and my physio. It was always diagnosed as Piriformis or Gluteus Recently the pain worsened after I had done certain exercises. The doctors expert in spine and also Ortho checked me and told me that I have no problem with my spine . I was asked any way to take an MRI.
Following is the result from the MRI : Diffuse bulge of L4-5 disc indenting the thecal sac and compromising the neural foramina.
Mild thickening of ligamentum flava is also noted at this level.
? Early lumbar spondylosis .
I have no pain when I walk or sit but aggravates in certain positions and radiates down. Can I bend, Jog and also do certain stretches. Please advise on the extensions to be done and how bad is this.
Author
Thanks for your question Vijay. You shouldn’t do stretches or jogging for now. Try these exercise only nothing else https://www.bodiempowerment.com/herniated-disc-part-2-the-best-exercises-for-your-herniated-disc/
The exercise should be supervised by a health professional. If the exercises give you more pain or make any symptoms go further down the leg than you should stop. Thing like numbness, tingling, or pain.
Hope that helps your disc hernaition.